This toolkit contains resources, tools, and examples to develop effective use cases for Health Information Exchange (HIE).

![]()
![]()
![]()
![]()
![]()
Use Case Library
This library contains Use Cases that improve care coordination, support Promoting Interoperability programs and implement other HIE goals. Each Use Case provides generalized guidance and you can use the Use Case Tools to tailor a case to your organization's needs. Many Use Cases are illustrated with a real-life example from an organization that implemented the case, and/or linked to a related HIE Spotlight Story.
The Use Cases are grouped into multiple tables by HIE Use Case category, including: Closed Loop Referrals, Summaries of Care, Discharge Summaries, Care Coordination, Lab Exchange, Query HIE, and Public Health Reporting.
Transitions of Care: Closed Loop Referrals
| Closed Loop Referrals | Objectives and Resources | |
|---|---|---|
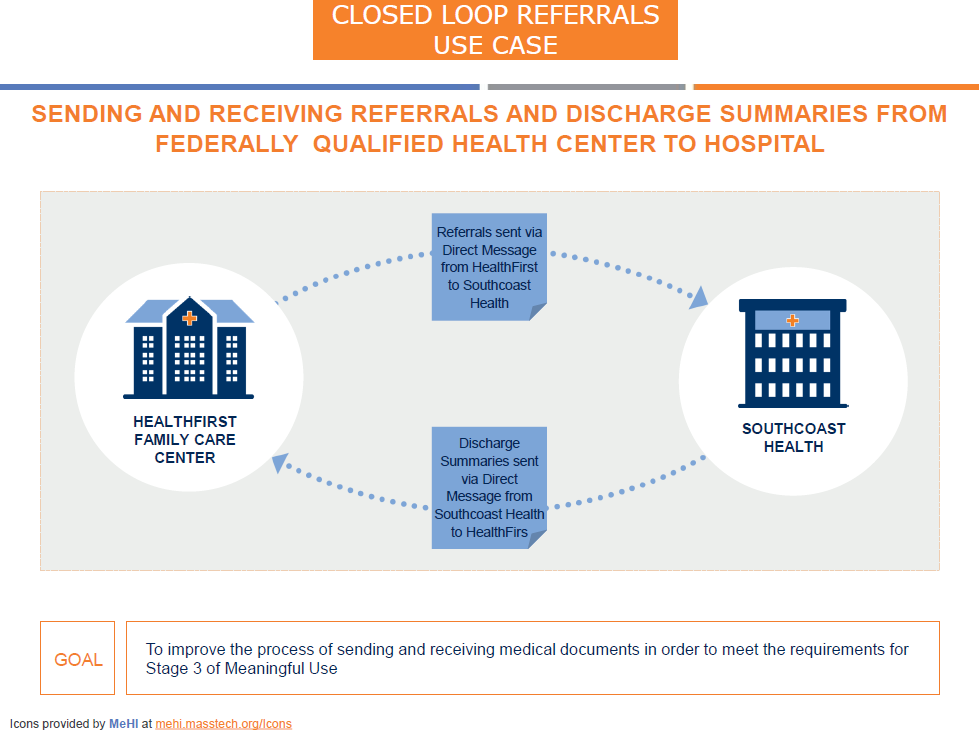
| Closed Loop Referrals from Federally Qualified Health Center to Hospital | ||
 |
| |
| ||
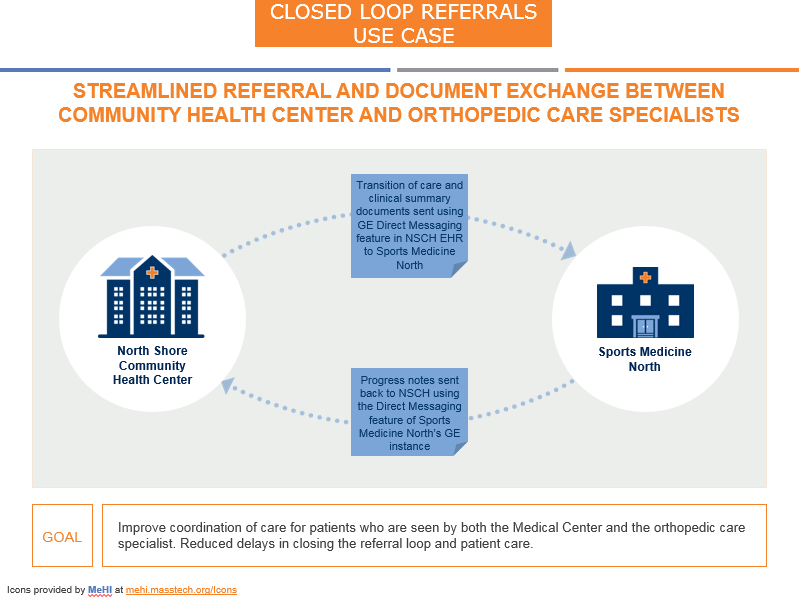
| Closed Loop Referrals from Community Health Center to Orthopedic Care Specialists | ||
 |
| |
| ||
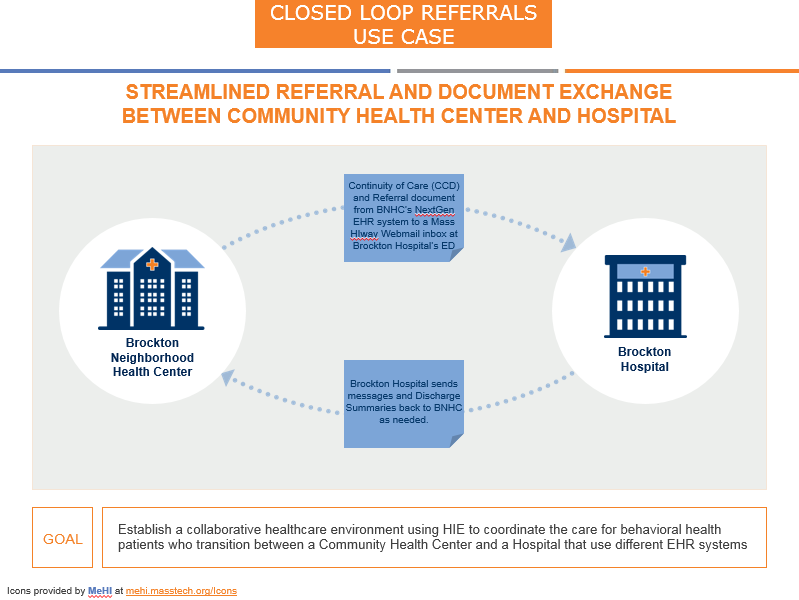
| Closed Loop Referrals from Community Health Center to Hospital | ||
 |
| |
| ||
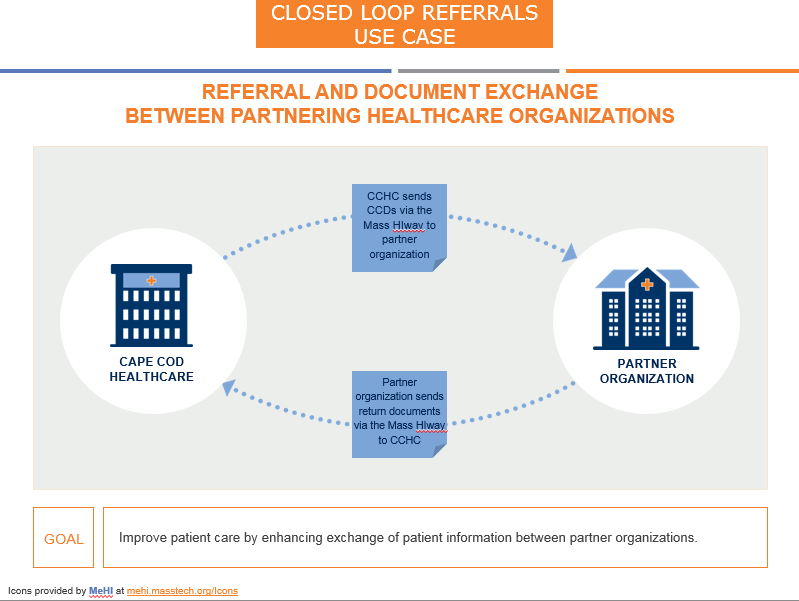
| Closed Loop Referrals between Partnering Organizations | ||
 |
| |
| ||
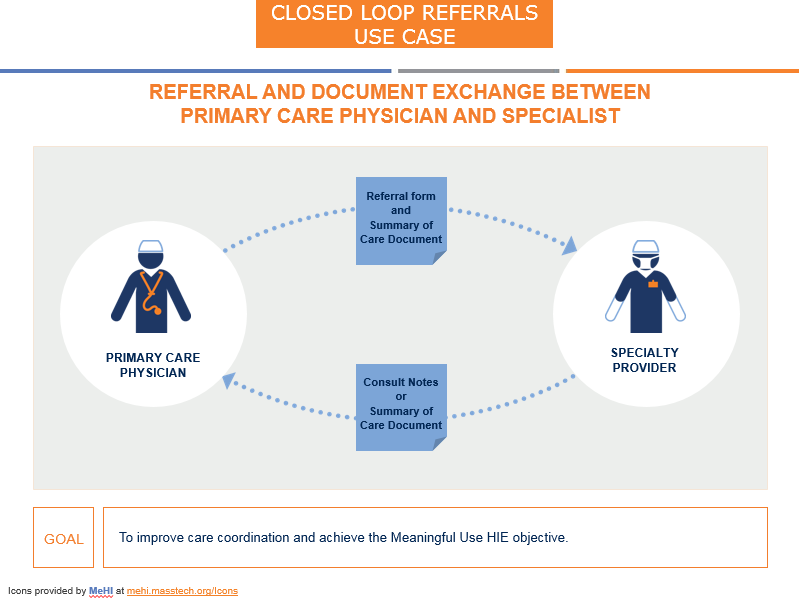
| Closed Loop Referrals from PCP to Specialist | ||
 |
| |
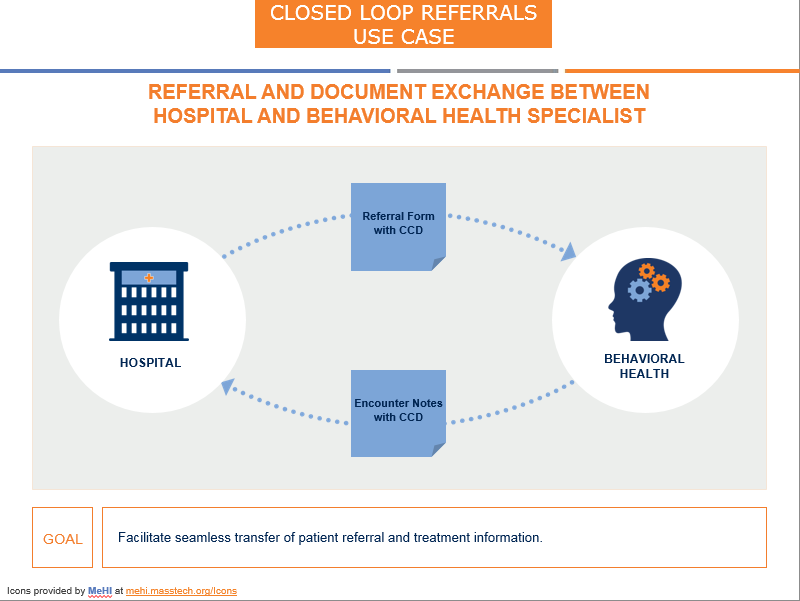
| Closed Loop Referrals from Hospital to Behavioral Health Specialist | ||
 |
| |
Transitions of Care: Summaries of Care
| Summaries of Care | Objectives and Resources | |
|---|---|---|
| Summaries of Care from Community Health Center to Partner Hospitals | ||
 |
| |
| ||
| Summaries of Care from Hospital to Specialized Medical Center | ||
 |
| |
| ||
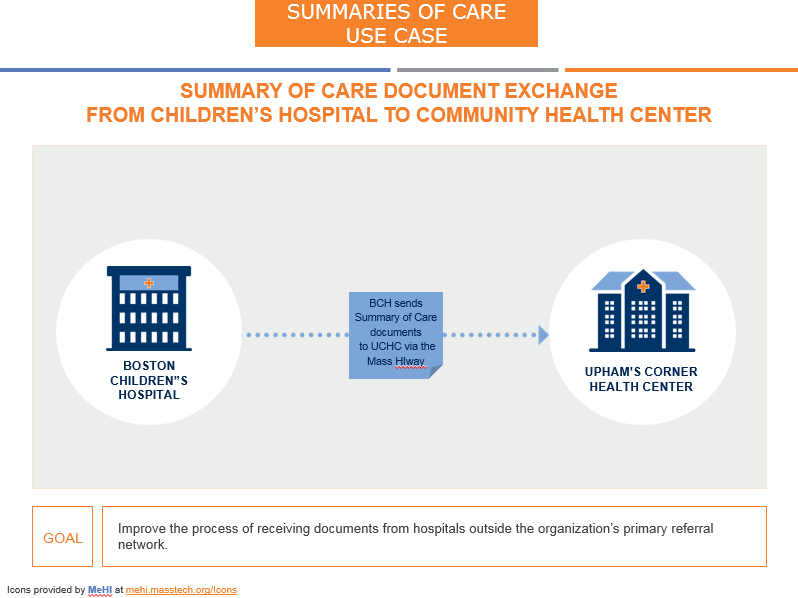
| Summaries of Care from Children's Hospital to Community Health Center | ||
 |
| |
| ||
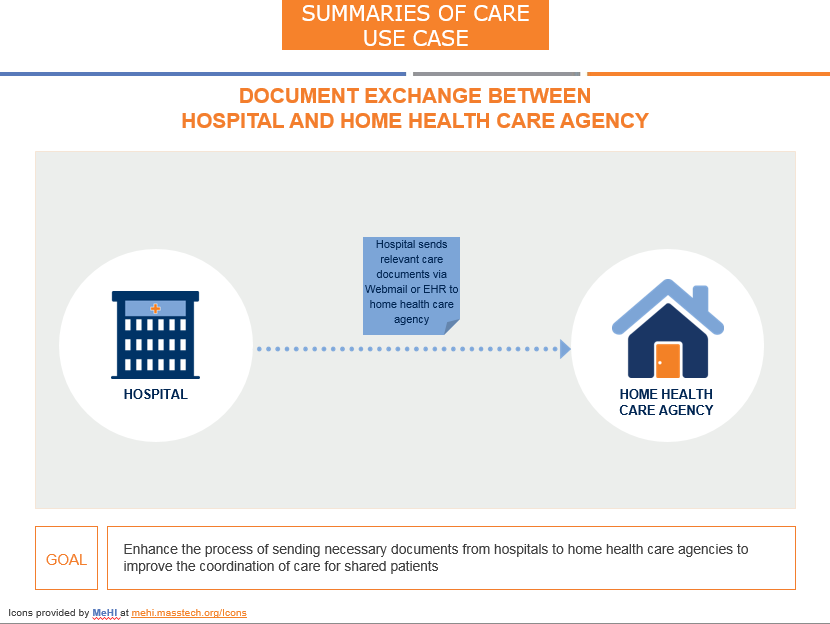
| Summaries of Care from Hospital to Home Health Care Agency | ||
 |
| |
| ||
| Summaries of Care from PCP to Behavioral Health Specialist | ||
 |
| |
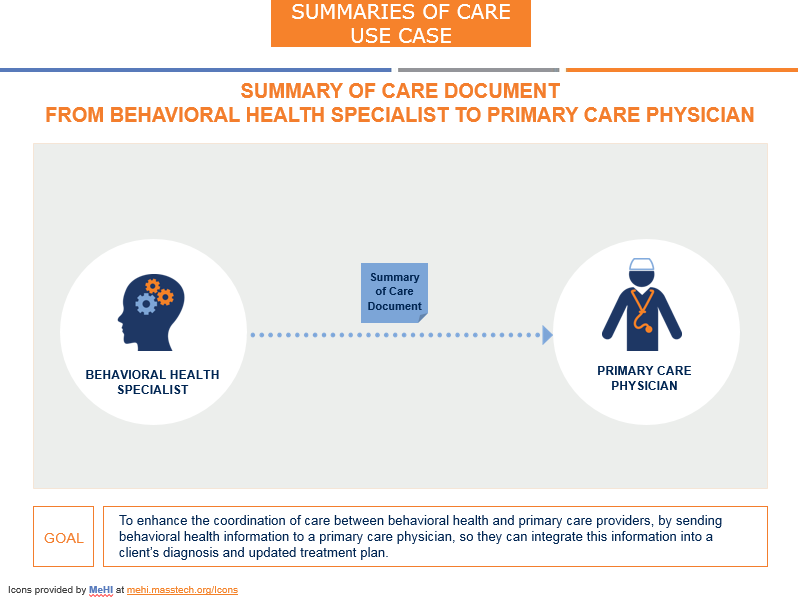
| Summaries of Care from Behavioral Health Specialist to PCP | ||
 |
| |
Transitions of Care: Discharge Summaries
| Discharge Summaries | Objectives and Resources | |
|---|---|---|
| Discharge Summaries from Hospital to Healthcare Practice | ||
 |
| |
| Discharge Summaries from Hospital to Post-Acute Care | ||
 |
| |
| ||
| Discharge Summaries from Rehab Center to Home Health Agency | ||
 |
| |
| ||
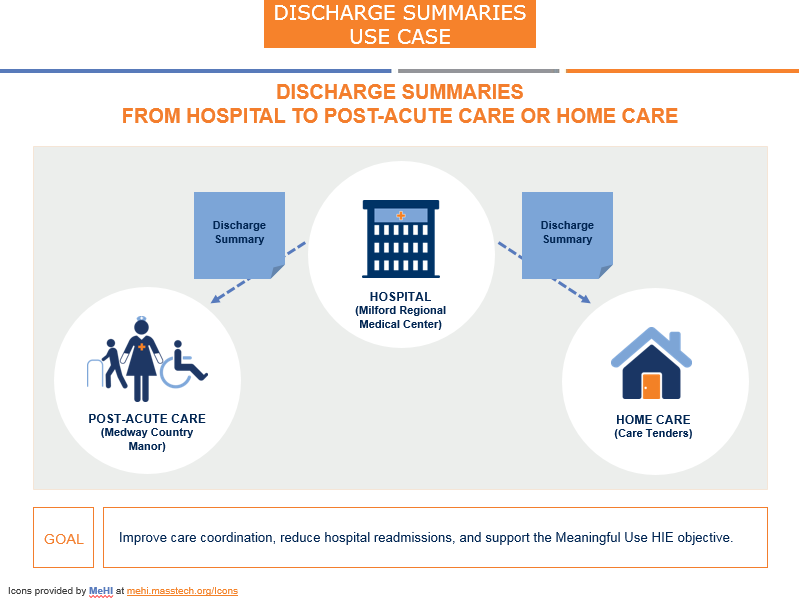
| Discharge Summaries from Hospital to Post-Acute Care or Home Care | ||
 |
| |
Care Coordination
| Care Coordination | Objectives and Resources | |
|---|---|---|
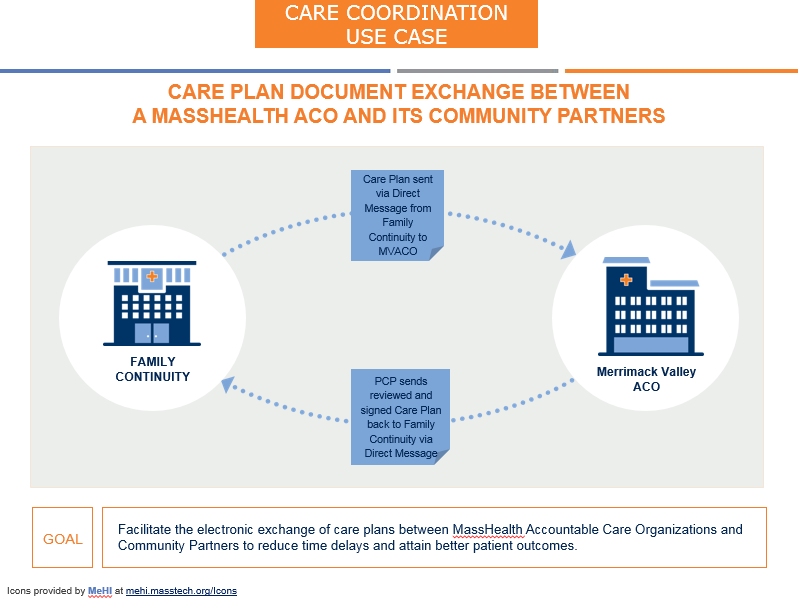
| Care Plan Document Exchange between a MassHealth ACO and its Community Partners | ||
 |
| |
| ||
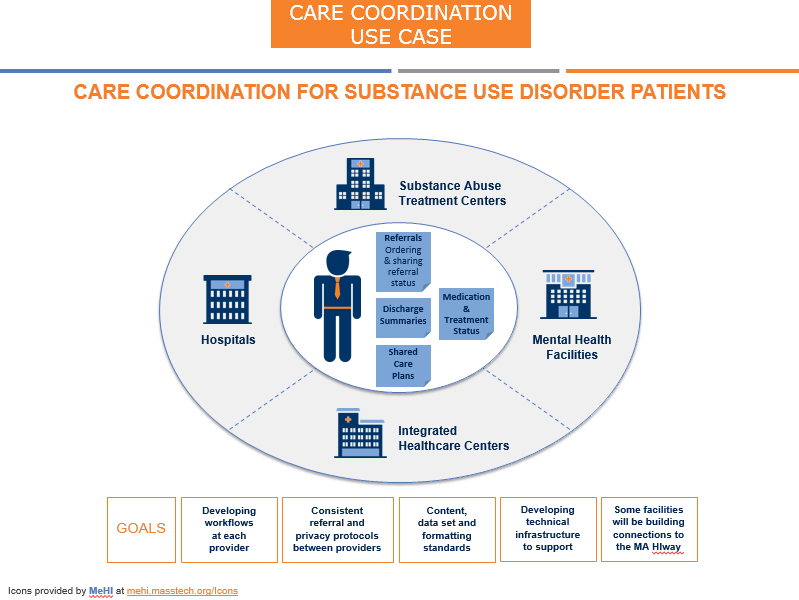
| Care Coordination for Substance Use Disorder | ||
 |
| |
| Care Coordination for Co-Occurring Acute Medical and Behavioral Health Conditions | ||
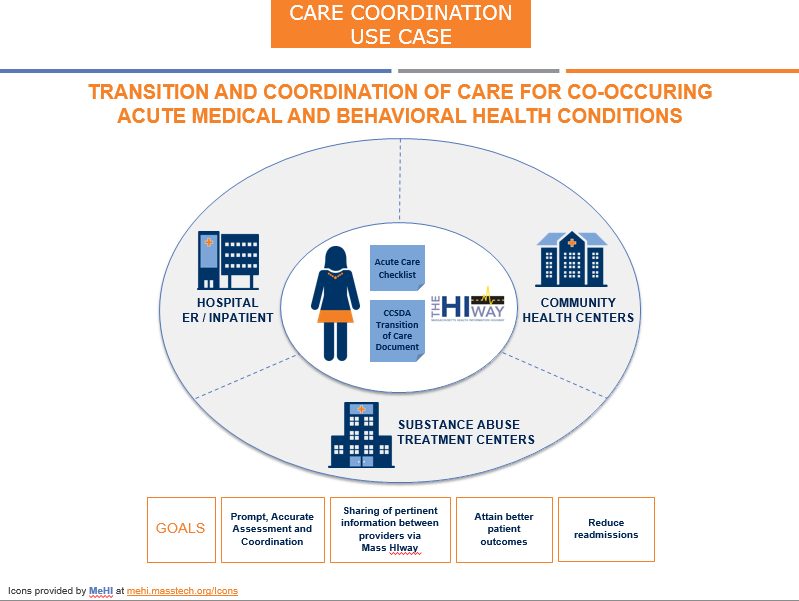 |
| |
| Care Coordination for Surgery between Orthopedic Specialty Provider, Hospital, and Home Care | ||
 |
| |
| Care Coordination between PCP and Behavioral Health Provider | ||
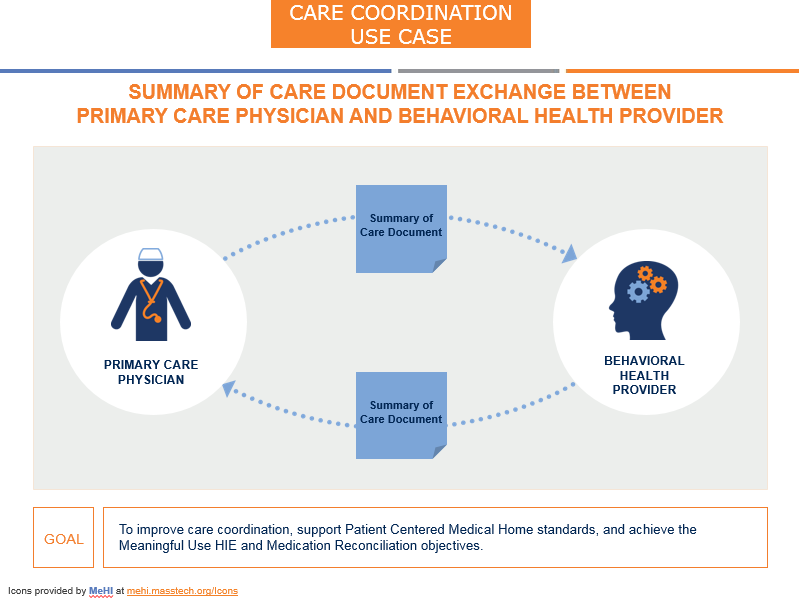 |
| |
Lab Exchange
| Lab Exchange | Objectives and Resources | |
|---|---|---|
| Exchange of Lab Order and Lab Results between Hospital Lab and Home Health Agency | ||
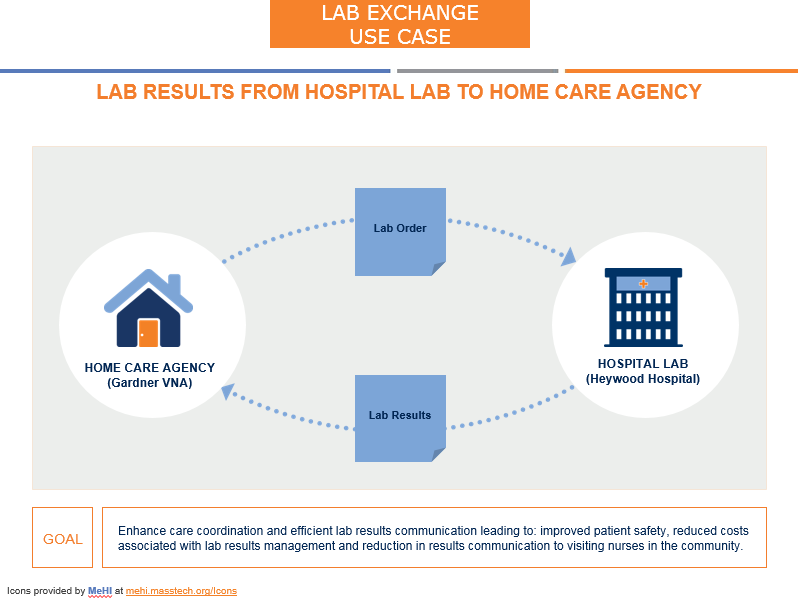 |
| |
Query HIE
| Query HIE | Objectives and Resources | |
|---|---|---|
| Customized Query HIE between Medical Group and Partnering Hospitals | ||
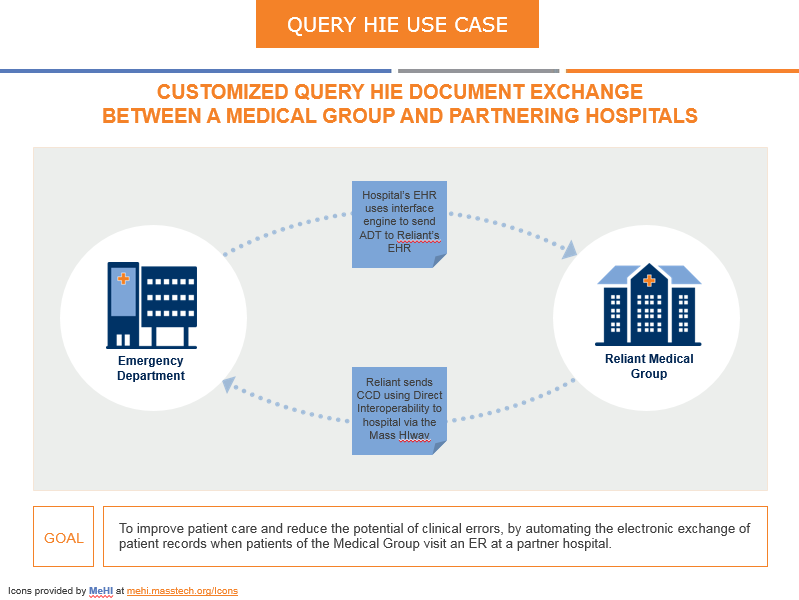 |
| |
| ||
Public Health Reporting
| Public Health Reporting | Objectives and Resources | |
|---|---|---|
| Child and Adolescent Needs and Strengths (CANS) Assessments from Community-based Organization to MassHealth | ||
 |
| |
| ||
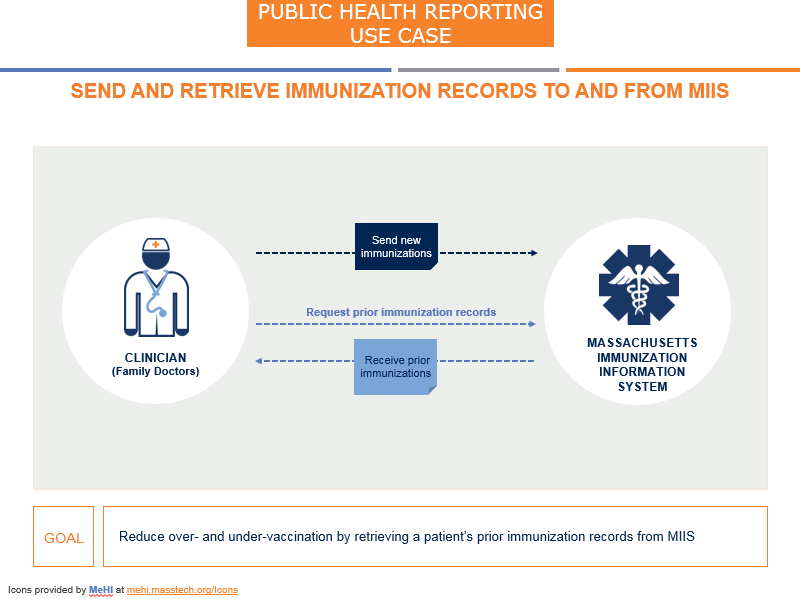
| Send and Retrieve Immunization Data to and from MIIS (Massachusetts Immunization Information System) | ||
 |
| |
| ||
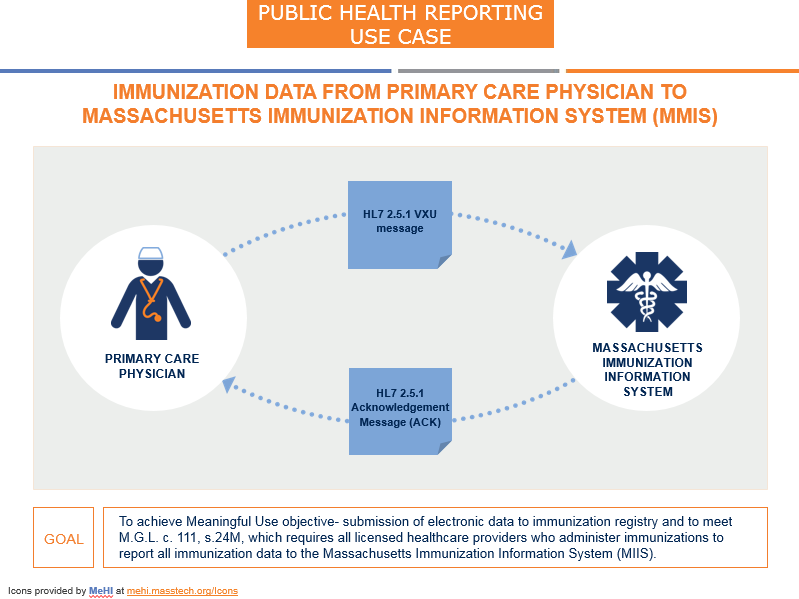
| Send Immunization Data to MIIS with Acknowledgement of Receipt | ||
 |
| |